Amde Selassie Shifera, MD, PhD
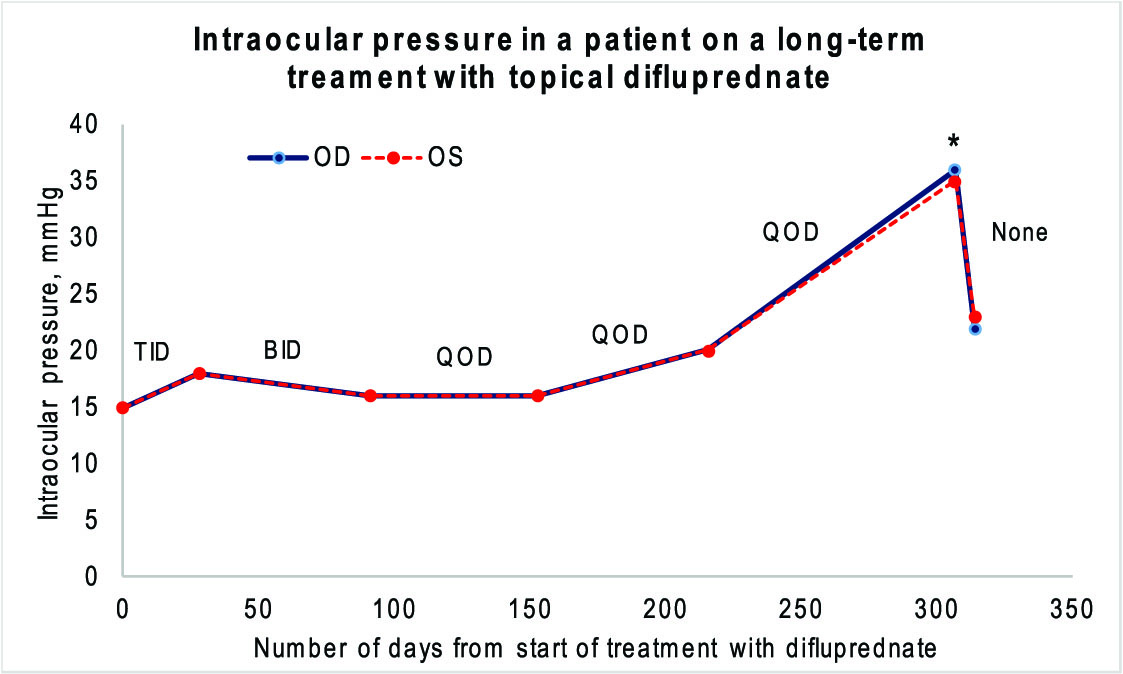
This is a brief case report to highlight the possibility of a delayed intraocular pressure elevation that can be associated with the use of 0.05% difluprednate (Durezol® Alcon, Fort Worth, TX). A 58-year-old white male who was being followed for bilateral idiopathic intermediate uveitis was started on difluprednate TID OU for the treatment of active vitritis. As the degree of the vitritis improved, the difluprednate was tapered down to QOD OU. His baseline IOP was 15 mmHg in each eye. He did not have a personal or family history of glaucoma. His IOP did not show any significant elevation till 307 days after starting difluprednate, when it was found increased to 36 and 35 mmHg OD and OS, respectively. (Fig. 1). At this point, with the inflammation suppressed, the difluprednate was stopped and the patient was started on dorzolamide HCl-timolol maleate BID OU. One week later, the IOP had decreased to 22 and 23 mmHg OD and OS, respectively.
Sorkin et al, who investigated the efficacy of 0.05% difluprednate in the treatment of graft rejection in patients with penetrating keratoplasty, highlighted that 21.2% of the eyes treated with difluprednate had IOP elevation with the range of timing of IOP elevation being 14-183 days.1 Moreover, they pointed out that a substantial portion of the IOP elevation was delayed.
Difluprednate is highly potent steroid, with its anti-inflammatory activities being 66 times that of cortisol as demonstrated using the granuloma pouch test in rats.2 Although the high potency of difluprednate makes it attractive for the treatment of ocular inflammation including corneal graft rejection, its use is fraught with a high risk of ocular hypertension. Currently, there are no guidelines as to how often and how long the IOP should be monitored. But, as evidenced in this letter and also in the study by Sorkin et al,1 the elevation of IOP can be delayed. As such, it is highly prudent to monitor the IOP regularly while a patient is on difluprednate regardless of the duration of use.
References
1. Sorkin N, Yang Y, Mednick Z, et al. Outcomes of difluprednate treatment for corneal graft rejection. Can J Ophthalmol 2020;55:82-86.
2. Dulin WE, Schmidt FL, Lyster SC. Biological activity of some 6 alpha-fluoro and 16 alpha-methyl C-21 steroids. Proc Soc Exp Biol Med 1960;104:345-8.
Amde Selassie Shifera, MD, PhD
Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, Maryland, USA (former address)