Optical coherence tomographic findings in Terson syndrome
Eric L. Crowell, MD, MPH*†Amde Selassie Shifera, MD, PhD*
Running title: OCT in Terson syndrome
From the *Wilmer Eye Institute, Johns Hopkins University School of Medicine, Baltimore, Maryland
†Current address: University of Texas Health Sciences Center at Houston, Houston, Texas
Reprint requests: Amde Selassie Shifera, MD, PhD, 600 N. Wolfe St, Woods Building, Room 471, Baltimore, MD 21287. TEL: 410-955-1966. E-mail: ashifer3@jhmi.edu
Conflict of interest: The authors have no conflict of interest to disclose.
Source of funding: AS is supported an institutional grant to the Wilmer Eye Institute from Research to Prevent Blindnessand by donations from grateful patients.
Keywords: intraretinal hemorrhage; optical coherence tomography; subretinal hemorrhage; sub-internal limiting membrane hemorrhage; Terson syndrome
Summary statement: Optical coherence tomography was used to demonstrate the multi-layered retinal hemorrhage that developed in the macula of a patient with Terson syndrome and to evaluate the change in the appearance of the hemorrhage over time.
A 62-year-old man presented with a 5-day history of central scotoma of his left eye. Five days prior to presentation he hit his head against the bottom of a trailer. Approximately 30 minutes after the accident he noticed a dark grayish spot in the center of his vision. He also reported that when looks at a light source the light would look reddish. The patient also reported having a generalized headache of a moderate degree that lasted for 15 minutes after the accident.
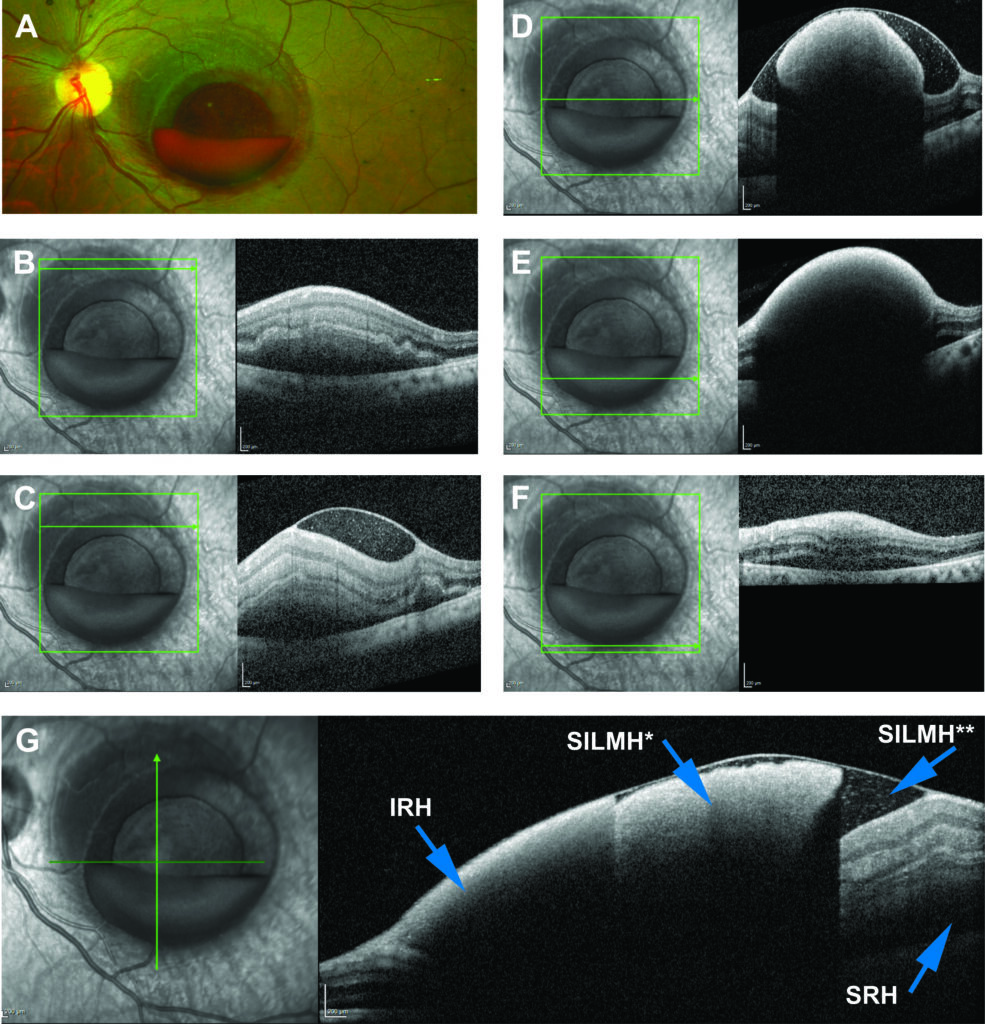
At presentation, his visual acuity in the left eye was counting fingers at 3 feet. On examination he was found to have a layered hemorrhage in the macula of the left eye (Figure 1A). Spectral domain optical coherence tomography (OCT; Spectralis system; Heidelberg Engineering) showed multi-layered hemorrhagein the macula of the left eye.Specifically, the OCT showed sub-internal limiting membrane (ILM) hemorrhage (both clotted and non-clotted), intraretinal hemorrhage and subretinal hemorrhage (Figure 1B to G). Examination of the right eye was non-remarkable. A computed tomography of the head done at presentation did not show any evidence of intracranial hemorrhage. No intervention was done at the initial presentation.
REFERENCES
1. Augsten R, Konigsdorffer E and Strobel J. Surgical approach in terson syndrome: vitreous and retinal findings. Eur J Ophthalmol 2000; 10:293-296.
2. Biousse V et al. The ophthalmology of intracranial vascular abnormalities. Am J Ophthalmol 1998; 125:527-544.
3. Gress DR, Wintermark M and Gean AD. A case of Terson syndrome and its mechanism of bleeding. J Neuroradiol 2013; 40:312-314.
4. Kapoor S. Terson syndrome: an often overlooked complication of subarachnoid hemorrhage. World Neurosurg 2014; 81:e4.
FIGURE LEGENDS
Fig. 1. Images of the left eye at presentation. A. Pseudocolor fundus photograph of the left eye (Optos ultra-widefield imaging device; Optos, Marlborough, MA). B to F. Horizontal optical coherence tomographic scans through the macula of the left eye. G. A vertical optic coherence tomographic scan through the macula of the left eye. IRH, intraretinal hemorrhage; SILMH*, clotted sub-internal limiting membrane hemorrhage; SILMH**, non-clotted sub-internal limiting membrane hemorrhage; SRH; subretinal hemorrhage.
Fig 2. Optical coherence tomography of the left eye one month after presentation. A. A horizontal scan through the macula. B. A vertical scan through the macula.